
Part II. Turning A Probable Death Sentence Into A Manageable Risk
Welcome back!
Lets begin by addressing the last question from Part I: Who should get screened for colorectal cancer, if anyone at all?
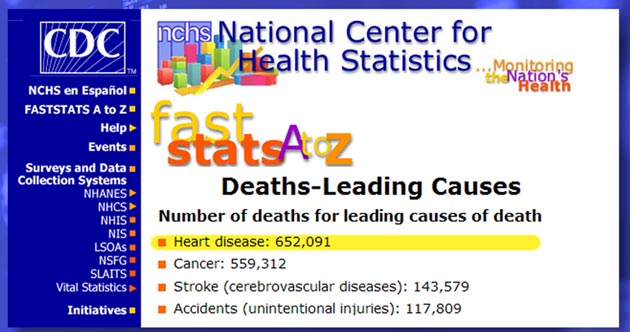
Well, for starters, lets keep the mortality rate from colorectal cancer in perspective. Even a person in a high-risk group is 12 times as likely to die from heart disease; 10 times — from any other cancer, 6 times — from a medical error [13], 3 times from stroke, and twice as likely to die from an accident… [14]
Considering these stats, the paranoia whipped up by Ms. Couric and her paymasters wasn't, obviously, about saving your life, but about making a buck.
You have also learned by now that regular screenings 5 or 10 years apart are more or less useless, and, adding insult to injury, that virtual colonoscopies may cause all kinds of other cancers.
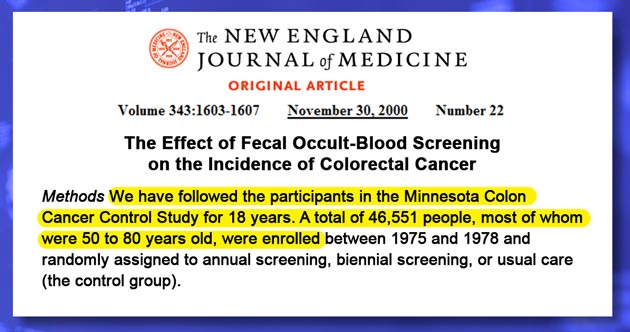
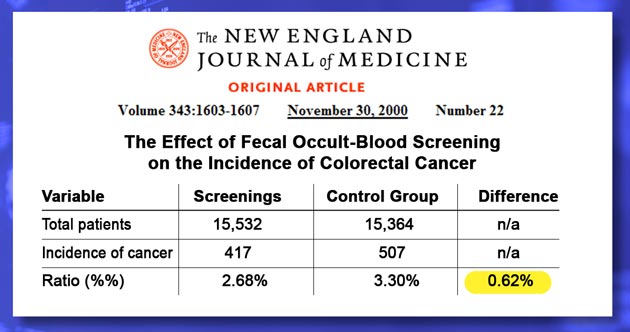
But even if you ignore all these facts, and decide to get screened as often as every year, consider the outcome of the Minnesota Colon Cancer Control Study [15]. It included 46 thousand patients between the ages of 50 and 80 and lasted for a whopping 18 years.
But in the end, it demonstrated only 0.62% reduction in the incidence of colorectal cancer. Statistically speaking, a difference this tiny was purely a chance happening.
Another prominent trial, known as the Telemark Polyp Study I [16], have been equally discouraging. The absolute difference in the incidence of colorectal cancer between screened patients and controls was only 2%, while the mortally rate from all causes in the screened group was 157% higher than among those who hadn't been screened (In the video I mistakenly indicate 57% instead of 157% — KM) .
Here is what it all means: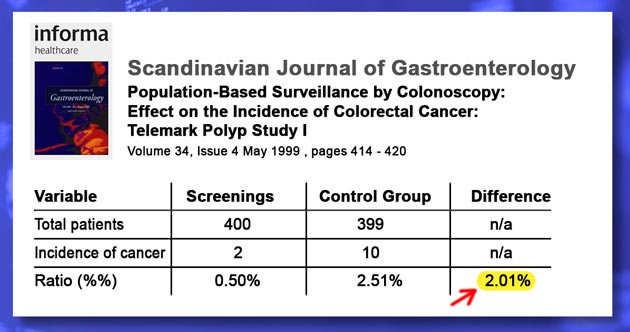
— First, If you are in a low-risk group, regular screenings will very likely increase your chances of death or disease from all other causes;
— Second, If you are in a high-risk group, even annual screenings aren't materially helpful.
— And third, if screenings are indeed useless, then a strategy of life-long prevention is the only viable way to escape colorectal cancer, especially for high-risk individuals.
These three conclusions bring up three equally crucial questions:
— First, how do you determine if you or your loved ones are at risk?
— Second, is it actually possible to prevent colorectal cancer?
— And, third — if it is, indeed, possible to prevent it, what should you do?
So lets address the first question first:
— Are you or your loved ones in the high-risk group for colorectal cancer?
I know the answer to this question better than most because I myself have a genetic predisposition to colorectal cancer through my Ashkenazi Jewish heredity and a long history of colorectal disorders. Also, my wife's dad had colon cancer, and this places Tatyana in the high risk group too. And both of us are well past fifty.
Considering this backdrop, we are just as scared as anyone would be in our shoes. So, if you are a confirmed hypochondriac, you may definitely pursue safe and non-invasive stool tests for colon cancer markers as often as you like.
Stool Tests For Colon Cancer Markers:
— Guaiac [pronounced gwahy-ak] fecal occult blood test (gFOBT);
— Stool DNA test (sDNA);
— Fecal immunochemical test (FIT)]
If these tests prove positive or there are any unexplained symptoms, you should definitely undergo conventional colonoscopy.
And now, lets address the next question:
— Is it possible to prevent colorectal cancer?
Absolutely! The majority of colorectal cancers aren't hereditary, and the majority of people in the high-risk group never develop one either. This means that colorectal cancer is connected to lifestyle factors just like lung cancer is connected to one's smoking. Eliminate these risk factors, and you'll reduce your chances of getting hit with colorectal cancer for the same reasons not smoking reduces the risk of lung cancer. This ain't rocket science, that's for sure…
Just like with any other cancer, this is not a foolproof enterprise, but for anyone in the high risk group, a strategy of life-long prevention turns a probable death sentence into a manageable risk, and for anyone in the low risk group it just about eliminates the possibility.
Finally, lets address the last question:
— What should you do to eliminate as many risks of colorectal cancer as humanly possible?
There are several external, and, therefore, well-controllable risk factors. They are, respectively: wrong diet, malnutrition, poor bowel habits; side effects of drugs; poor immunity; common colorectal disorders, such as IBS, inflammatory bowel disease; damaged intestinal flora, and some others. To a large extent, all of them are interdependent. This means fixing one positively affects the rest, while neglecting one makes all others more damaging.
To sort out and eliminate all of these risks, please visit my web site GutSense.org. In addition to colon cancer prevention, it also addresses chronic constipation, diarrhea, irritable bowel syndrome, diverticular disease, and related complications. These widespread disorders commonly precede polyposis — the formations of polyps that may eventually turn into deadly tumors.
Obviously, to prevent polyposis, you must eliminate these conditions first. Otherwise, you can zap polyps all you want, but as long as their causes are still there, new ones will pop-up long before your next screening. That, essentially, explains why colonoscopies are so ineffective.
The most tragic aspect of this sad story is also the deadliest… The promoters of this fraud continue to intimidate unsuspecting Americans and their well-meaning doctors into the false belief that 'screening colonoscopies' are the only viable way of preventing colorectal cancer:
Voice of Katie Couric from March, 2007 video [YouTube link]:
“A colon is it's own container. If you can remove the polyp, even before it's cancerous, then you literally nip the disease in the bud.”
Voice of Konstantin Monastyrsky:
For goodness sake, Ms. Couric, please stop lying! The truth is (the following four slides displayed while Konstantin reads highlighted sections) :
From the National Cancer Institute web site [17]:
“…it is not yet known for certain whether colonoscopy can help reduce the number of deaths from colorectal cancer.”
From 'A Cancer Journal for Clinicians' [18]:
“…There are no prospective randomized controlled trials of screening colonoscopy for the reduction in incidence or mortality of CRC [colorectal cancer - KM].”
From The New York Times [19]:
“The patients in all the studies had at least one adenoma detected on colonoscopy but did not have cancer. They developed cancer in the next few years, however, at the same rate as would be expected in the general population without screening.”
From the Annals of Internal Medicine [20]:
“A goal of avoiding all deaths from colon cancer may be admirable, but we do not have evidence that we can achieve it.”
“Colonoscopy is an effective intervention, but, as Baxter and colleagues suggest, we must realize that current evidence is indirect and does not support a claim of 90% effectiveness.”
As a result, most people over fifty do nothing to materially prevent it, except praying for the best, and waiting in fear for yet another useless screening that may harm them even more.
I hope this isn‘t you!
Thank you for watching!
I wish you and your family good luck and good health!
References
13D. W. Bates; et al.; Incidence of adverse drug events and potential adverse drug events. Implications for prevention. ADE Prevention Study Group JAMA. 1995;274(1):29-34. [link]
14FASTSTATS A to Z; National Center for Health Statistics, Centers for Disease and Prevention; [link]
15Mandel, J, at al.; The Effect of Fecal Occult-Blood Screening on the Incidence of Colorectal Cancer; N Engl J Med 2000 343: 1603-1607 [link]
16Thiis-Evensen E, et al.; Population-based surveillance by colonoscopy: effect on the incidence of colorectal cancer. Telemark Polyp Study I.; Scand J Gastroenterol. 1999 Apr;34(4):414-20. [link]
17Colorectal Cancer Screening; National Cancer Institute; Oct 2008; [link]
18Levin, B., at al.; Screening and Surveillance for the Early Detection of Colorectal Cancer and Adenomatous Polyps, 2008: A Joint Guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology CA Cancer J Clin 2008 58: 130-160 [link]
19Study Questions Colonoscopy Effectiveness; The New York Times; G. Colata; Dec 14, 2006; [link]
20Ransohoff, D.; How Much Does Colonoscopy Reduce Colon Cancer Mortality? Ann Intern Med 2008; 60520-308. [link]