
Colon cancer prevention guide
Step 1. Normalize abnormal stools
The majority of adult Americans “carry around” 10 to 20 lb of formed stools inside their bowels instead of the 1 to 2 lb of semi-soft feces as the mother-nature meant it to be. This pathology is behind the raging epidemics of bowel disorders and colorectal cancer in the United States. Thus, reducing the size, weight, and density of stools to the norm, and keeping them this way for the rest of your life, is the most important and effective step toward the goal of preventing colorectal cancer.
Source: Wikipedia; licensed under the Creative Commons [link]
Large and heavy stools cause bowel disorders that precede colon cancer for the same reasons large and deep potholes ruin your car's suspension — accelerated wear-and-tear.
While your body is still young and resilient, it can handle the “potholes” with relative ease. But as it ages and loses its firmness and suppleness, the bowel transforms itself to accommodate “heavy luggage.”
This transformation, though, comes with a heavy price: bowel enlargement, diverticular disease, enlarged internal hemorrhoids, anorectal nerve damage, motility inertia, and the ensuing accumulation of impacted stools inside the colon that leads to irregularity and/or constipation. The colorectal polyps, lesions, and tumors complete this chain of events, with the brunt of the “breakdowns” commencing after the age 50.
Alas, you can't replace the colon to support the aging body the same way you can replace the shock absorbers to support the aging car. You can, however, “extend the warranty” by reducing stool size, weight, and density in the same way driving around potholes extends the life of your car.
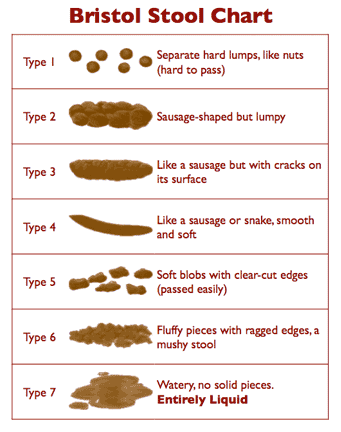
To check out what stools qualify as “large,“ and what not, look at the chart on the left. If yours looks like type 2 or 3, you are in “deep shit”, literally and figuratively. It means that your feces are impacted throughout the entire length of your large intestine all the way up to the blind gut, especially type 2. You can learn more about the Bristol Stool Chart, and what it means here.
Impacted stools require substantial physical effort (straining) to eliminate them. The resulting pressure on the delicate and narrow anal canal causes anal tears (streaks of blood on stools), nerve damage (loss of urge sensation), and enlarged internal hemorrhoids (pain during defecation) as these large stools pass the anal canal.
As these conditions progress, defecation becomes more and more difficult, painful, and incomplete, increasing the size of stools even more. As the stools' size and volume grows further, impacted stools stretch out the colon, and cause diverticulosis.
Near permanent contact of large stools such as type 2 and 3 with the inner wall of the large intestine causes inevitable inflammation, strips down the mucus lining when moving down and out, and contributes to the formation of polyps and lesions.
Bloating, cramping, severe flatulence, and occasional diarrhea are markers of this condition. Normally, the colon absorbs most of the fermentation-related gases back into the blood stream for release via the lungs. Inflammation of the mucosal membrane, however, blocks their absorption. Lacking an immediate escape, trapped gases expand the colon. This expansion, in turn, causes outward bloating and painful cramping.
A more severe bowel inflammation also blocks the absorption of fluids that continuously drip down from the small intestine. When the volume and pressure of fluids exceeds the holding capacity of the large intestine and they reach the rectum, the victim experiences profuse diarrhea. The resulting release of impacted stools allows temporary respite until the vicious cycle of irregularity —> more fiber —> stool enlargement —> mucosal inflammation —> diarrhea resumes again.
While all these drudgery is taking place, one day you may end up in the doctor's office with a sharp abdominal pain, most likely related to diverticular disease. After reviewing the results of your colonoscopy report or CT scan (adding yet another dose of cancer-causing radiation), your doctor will recommend more fiber to bulk up your already large stools, and more exercise to strengthen your abdominal muscles, so you can strain with even more force!
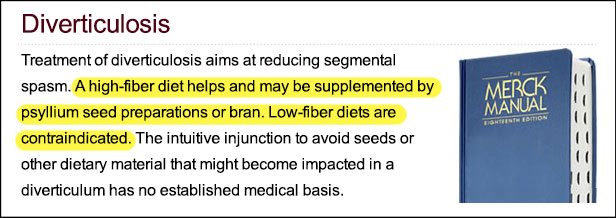
I am not making any of this up. Here is a verbatim description of this protocol courtesy of The Merck Manual [link]:
If you follow this advice, you are practically guaranteed to end up one day in the hospital with acute diverticulitis, or colon perforation, or appendicitis, or a prolapsed rectum, or internal bleeding, or something else just as bad.
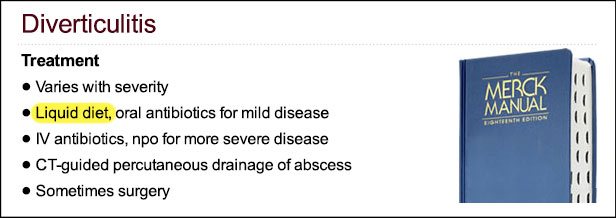
The moment you are admitted, doctors begin treatment by immediately putting you on a fiber-free, liquid diet, so you can (finally) recover. If you are really messed up, CT scans are ordered again, or surgery to cut out the affected portions of your large intestine [link]:
As you leave the hospital, your doctors will recommend that you resume a high-fiber diet again as soon as you heal:
And so it goes on until colectomy or colorectal cancer, whichever comes first, assuming you don‘t succumb first to stroke, heart attack, chest infection, kidney failure, or any other cancer as a result of blood loss, surgeries, general anesthesia, radiation, medication side effects, severe stress, or medical errors.
To avoid these risks, simply normalize your stools to the proper type 4 or 5 by following my recommendations in Restoring Natural Bowel Movement and Normalizing Stools page.
I accorded a disproportionate amount of attention to the discussion of diverticular disease for a simple reason: a localized inflammation of diverticulum is the most likely point of origin for precancerous lesions, polyps, and tumors. Correspondingly, diverticulosis is a marker for large stools, and represents one of the highest degree of risk for colorectal cancer.
According to the National Institute of Health, about half of all people over the age of 60 have diverticulosis [link]. The same age group happens to be affected by colorectal cancer the most. Do you see any connection?
If you have been already diagnosed with diverticular disease, and would like to spare yourself from related complications, follow my recommendations in the Diverticulosis and Diverticulitis page.
The following sentence was added to the Diverticulosis section of The Merck Manual in 2007 to, I believe, specifically respond to my analysis of the fiber-diverticulosis connection in Fiber Menace published two years earlier.
“The intuitive injunction to avoid seeds or other dietary material that might become impacted in a diverticulum has no established medical basis.”
The “no established medical basis” claim is incorrect. The fact is, by the time the affected colon is checked out by a radiologist or endoscopist for damage, it has already been thoroughly lavaged (cleaned out) from all stool, including impacted, hence the doctors will see nothing, but an unsoiled colon, whistle-clean intestinal walls, and empty diverticula.
Fiber Menace, actually, distinguishes between small and large diverticula, as well as soft and hard stools. Impaction of “dietary material” is only possible when either the affected diverticulum is large or the stools are hard and large. In all other cases, indeed, nothing can “become impacted.” Here is an actual excerpt from my book:
Diverticulosis starts developing during the latent stage of fiber-related constipation which, as you may recall, is primarily characterized by straining, hemorrhoids, and type 1–3 large stools on the Bristol Stool Form Scale. The smaller diverticula range in diameter from 3 mm to 3 cm, and are usually multiple. The ones that are really large are most likely single (the singular is diverticulum), and range in diameter from 3 to 15 cm. When fiber-laden feces get “diverted” into diverticula, they tend to get lodged there, and then lump together and harden up.
Diverticulosis can be reliably seen and diagnosed by radiography (X-ray, nuclear scan) or colonoscopy long before most patients experience any symptoms. Overall, smaller diverticula are harmless, as long as feces remain small, soft, and moist, because fecal matter with these properties won‘t get trapped inside small crevices.
But when feces are continuously large, hard, and dense, they may keep even tiny diverticula clogged indefinitely for the same reasons a tight cork keeps liquid inside a vessel turned upside down, even if the neck has multiple crevices on the inside.
As more and more fecal matter gets jam-packed inside each diverticulum, they may enlarge further by the sheer force of outward pressure. Eventually, the epithelium inside one or more diverticulum gets lacerated and infected. The infection may cause inflammation, ulceration, rectal bleeding, excruciating pain, and/or the perforation of the colon wall—collectively called diverticulitis.
Chapter 7, Diverticular Disease;
Fiber Menace, page 146
If you still doubt my analysis back from 2005 (when Fiber Menace was first published), thanks God, medical science isn't standing by. What I “squeaked” then, by now, has turned into the loud chorus:
Fiber Not Protective Against Diverticulosis
Contrary to popular medical wisdom, following a high-fiber diet has no protective effect against developing asymptomatic diverticulosis, according to a colonoscopy-based study presented at the 2011 Digestive Disease Week (DDW) meeting (abstract 275). In fact, the study showed that patients who ate more fiber actually had higher prevalence of the disease. [Gastroenterology and Endoscopy News, July 2011, Volume: 62:07]
Fiber May Not Prevent Diverticular Disease
For decades, doctors have recommended high-fiber diets to patients at risk for developing the intestinal pouches, known as diverticula. The thinking has been that by keeping patients regular, a high-fiber diet can keep diverticula from forming. But the new study suggests the opposite may be true. [WebMD, January 23, 2012]
A High-Fiber Diet Does Not Protect Against Asymptomatic Diverticulosis
A high-fiber diet and increased frequency of bowel movements are associated with greater, rather than lower, prevalence of diverticulosis. Hypotheses regarding risk factors for asymptomatic diverticulosis should be reconsidered. [Gastroenterology; Volume 142, Issue 2, Pages 266-272.e1, Feb. 2012]
If you are like “normal,” discussing the metrics of one's stool is a taboo not only between parents and their adult children, but also between spouses and siblings. Well, you don't have to... Instead, just click the button below to share this lifesaving information with the people you love.
Konstantin Monastyrsky